Predictors of Sarcopenia in Outpatients with Post-Critical SARS-CoV2 Disease. Nutritional Ultrasound of Rectus Femoris Muscle, a Potential Tool

 , ,
, ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design
2.2. Body Composition Analysis
2.2.1. Phase Angle by BIVA
2.2.2. Nutritional Ultrasound®
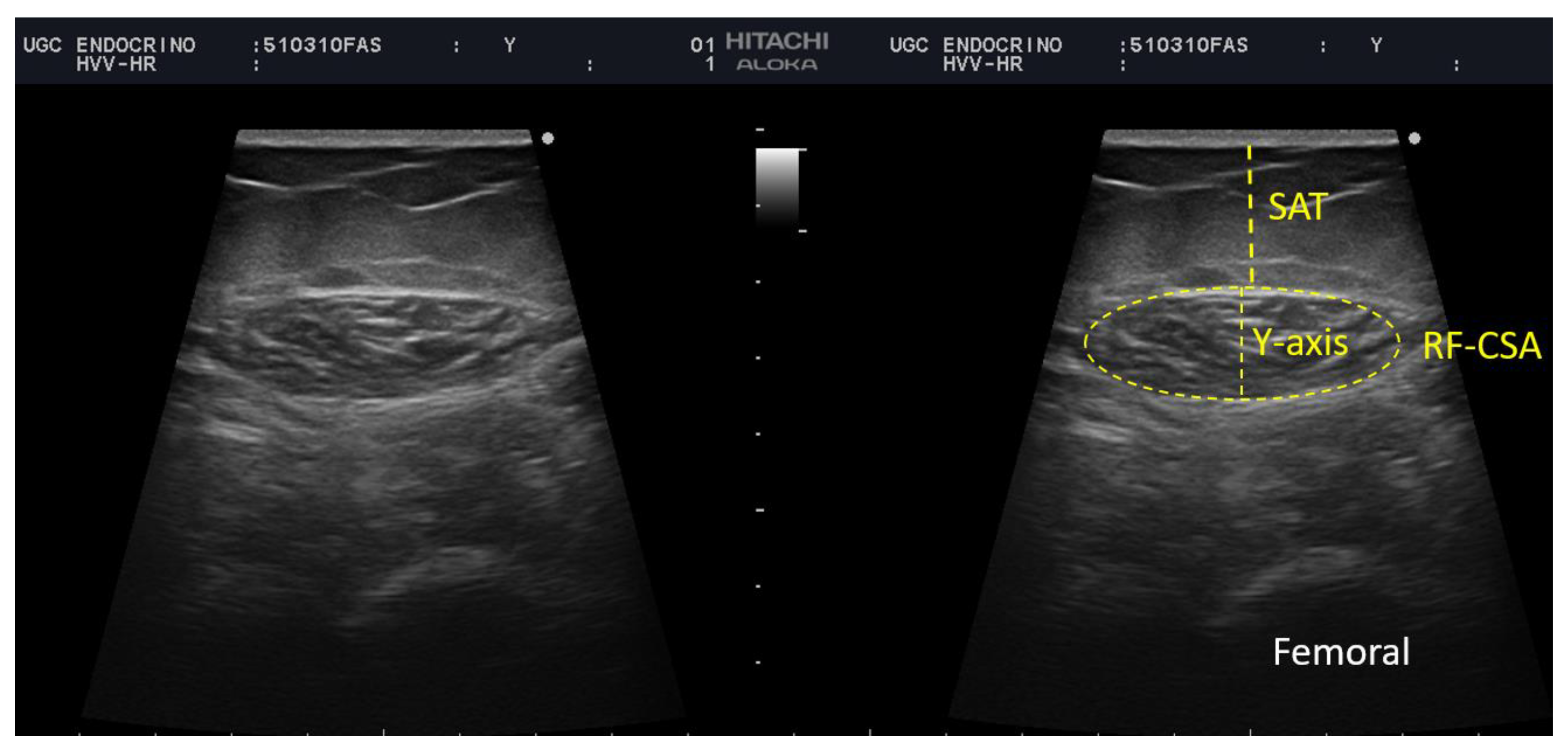
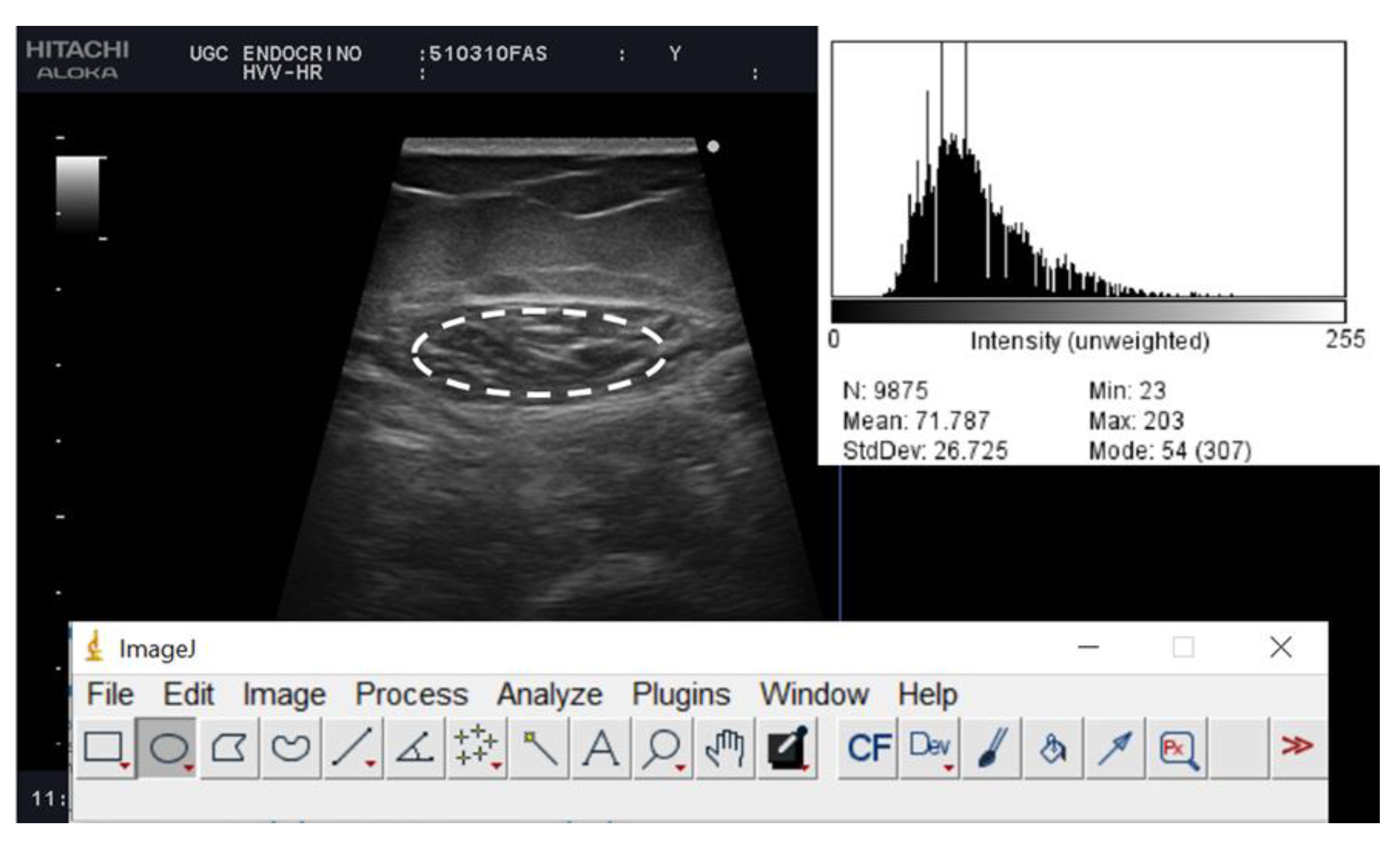
Rectus Femoris (RF) Ultrasound Assessment
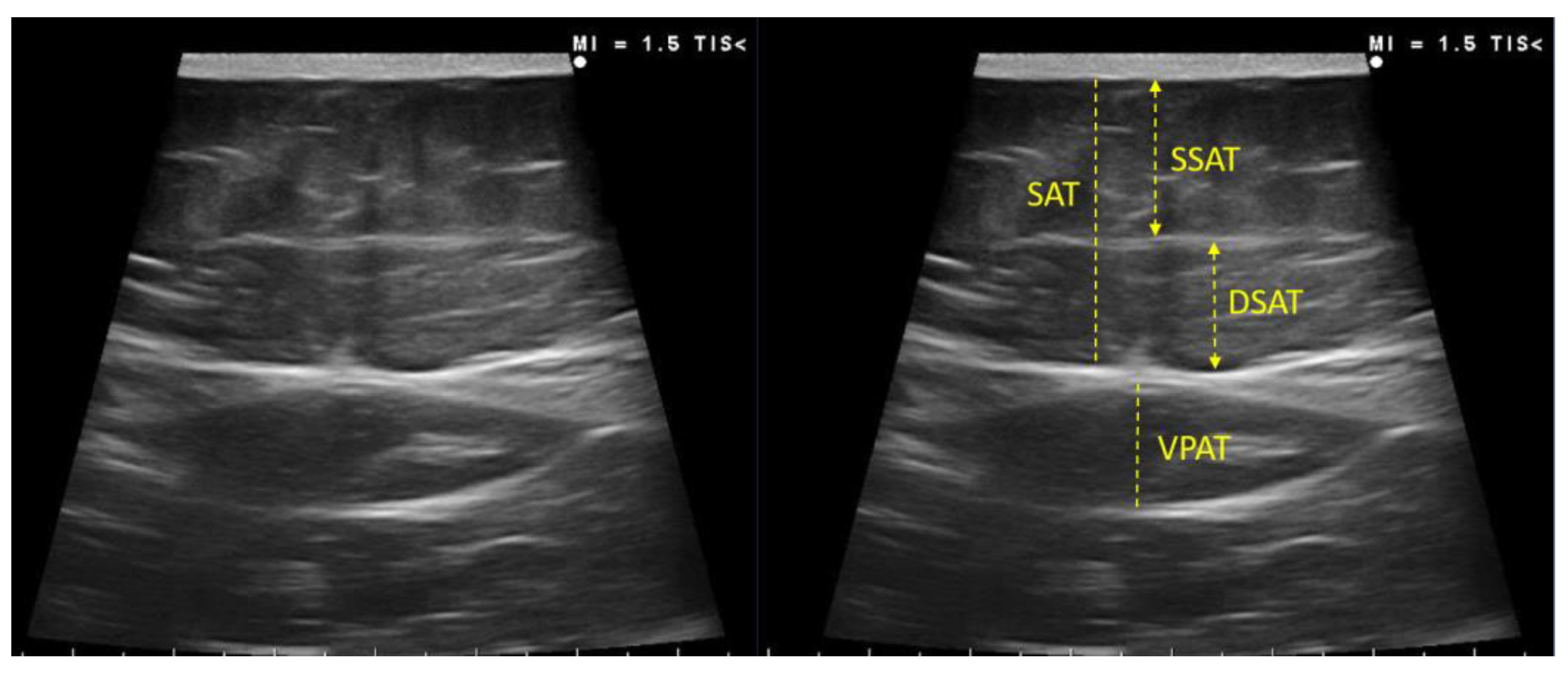
Adipose Tissue Ultrasound Assessment
2.3. Functional and Muscle Strength Assessment
2.4. Clinical Variables
2.5. Statistical Analysis
3. Results
3.1. Baseline Characteristics
3.2. Risk Factors of ICU Admission That Condition Muscle Mass (Sarcopenia)
3.3. BIVA Analysis and Body Composition Estimates for the Diagnosis of Sarcopenia and Excess Fat Mass
3.4. Ultrasound Evaluation of RF Muscle
3.5. Functional Status Assessment
3.6. Degree of Agreement between Body Composition Techniques (Bioelectrical Measurements and Muscle Ultrasound): Correlation of the New Ultrasound Values with the Validated Measurement of BIVA Parameters of COVID-19 Post-Critical Patients
3.7. Relationship between the Functional Aspects and Body Composition Techniques (Bioelectrical Measurements and Muscle Ultrasound)
3.8. Evaluation of Qualitative Characteristics of the Muscle, and Muscle Quality
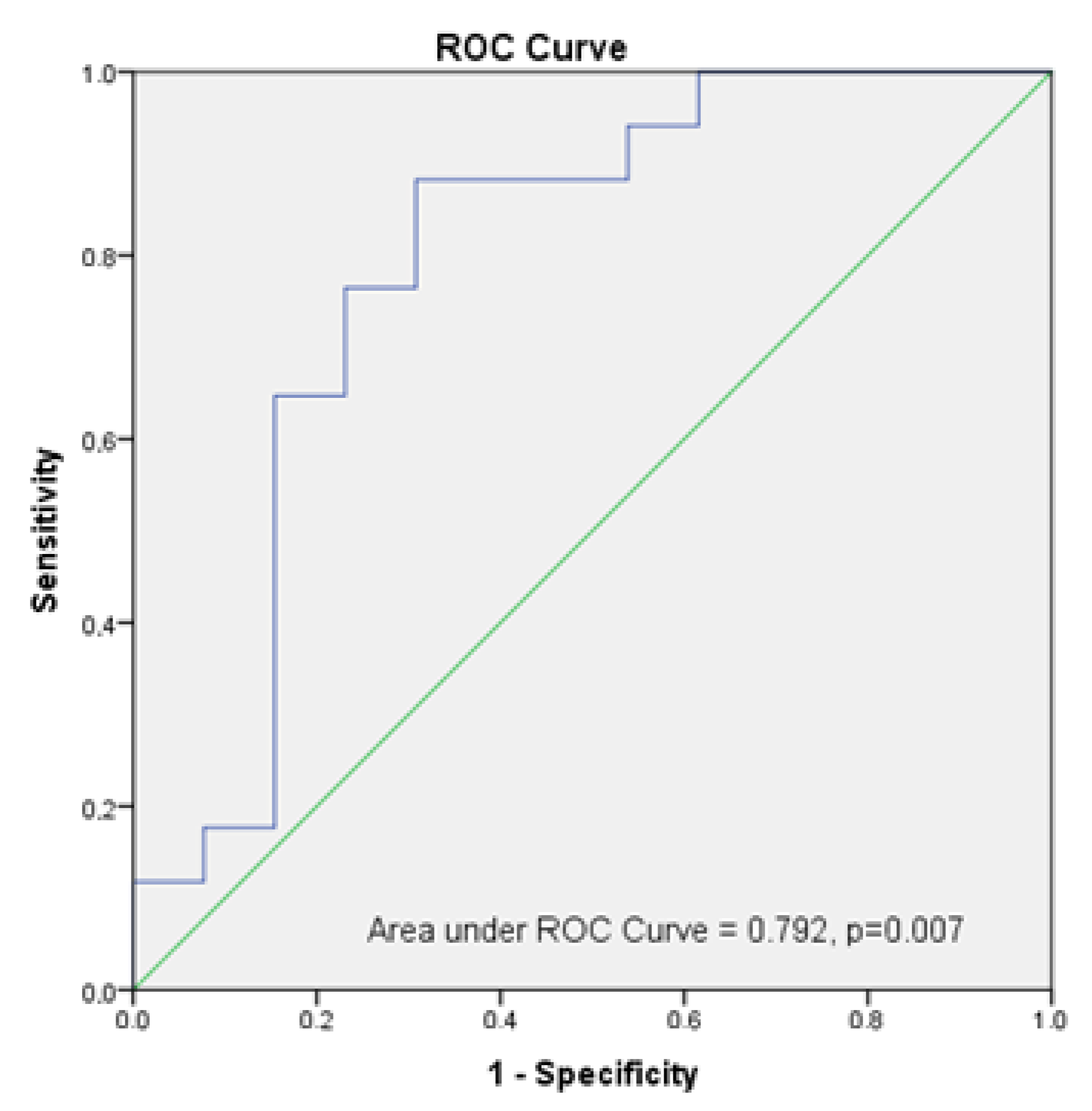
3.9. Establishment of Muscle Mass Estimation Algorithms and Cut-Off Value for Sarcopenia Diagnosis in Post-Critical COVID-19 Outpatients
4. Discussion
5. Limitations and Strengths
6. Conclusions
Supplementary Materials
Author Contributions
Funding
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- González-Salazar, L.E.; Guevara-Cruz, M.; Hernández-Gómez, K.G.; Serralde Zúñiga, A.E. Nutritional Management of the Critically Ill Inpatient with COVID-19. A Narrative Review. Nutr. Hosp. 2020, 34, 622–630. [Google Scholar] [PubMed]
- Andrade-Junior, M.C.D.; Salles, I.C.D.D.; de Brito, C.M.M.; Pastore-Junior, L.; Righetti, R.F.; Yamaguti, W.P. Skeletal Muscle Wasting and Function Impairment in Intensive Care Patients with Severe COVID-19. Front. Physiol. 2021, 12, 640973. [Google Scholar] [CrossRef] [PubMed]
- Cornejo-Pareja, I.; Vegas-Aguilar, I.M.; García-Almeida, J.M.; Bellido-Guerrero, D.; Talluri, A. Phase Angle and Standardized Phase Angle from Bioelectrical Impedance Measurements as a Prognostic Factor for Mortality at 90 Days in Patients with COVID-19: A Longitudinal Cohort Study. Clin. Nutr. 2020, in press. [Google Scholar] [CrossRef]
- Buckinx, F.; Landi, F.; Cesari, M.; Fielding, R.A.; Visser, M.; Engelke, K.; Dennison, E.; Al-Daghri, N.M.; Allepaerts, S.; Bauer, J.; et al. Pitfalls in the Measurement of Muscle Mass: A Need for a Reference Standard. J. Cachexia Sarcopenia Muscle 2018, 9, 269–278. [Google Scholar] [CrossRef] [PubMed]
- Maza, D.; Henriquez, S.; Berger, J.; Bunout, D.; Barrera, G.; Leiva, L.; Hirsch, S. Rectus Femoris (RF) Ultrasound for the Assessment of Muscle Mass in Older People. Arch. Gerontol. Geriatr. 2015, 61, 33–38. [Google Scholar] [CrossRef]
- Rustani, K.; Kundisova, L.; Leopoldo, P.; Nante, N.; Bicchi, M. Ultrasound Measurement of Rectus Femoris Muscle Thickness as a Quick Screening Test for Sarcopenia Assessment. Arch. Gerontol. Geriatr. 2019, 83, 151–154. [Google Scholar] [CrossRef] [PubMed]
- Mueller, N.; Murthy, S.; Tainter, C.R.; Lee, J.; Richard, K.; Fintelmann, F.J.; Grabitz, S.D.; Timm, F.P.; Levi, B.; Kurth, T.; et al. Can Sarcopenia Quantified by Ultrasound of the Rectus Femoris Muscle Predict Adverse Outcome of Surgical Intensive Care Unit Patients and Frailty? A Prospective, Observational Cohort Study Noomi. Ann. Surg. 2017, 264, 1116–1124. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hernández-Socorro, C.R.; Saavedra, P.; López-Fernández, J.C.; Ruiz-Santana, S. Assessment of Muscle Wasting in Long-Stay ICU Patients Using a New Ultrasound Protocol. Nutrients 2018, 10, 1849. [Google Scholar] [CrossRef] [Green Version]
- Donini, L.M.; Busetto, L.; Bischoff, S.C.; Cederholm, T.; Ballesteros-Pomar, M.D.; Batsis, J.A.; Bauer, J.M.; Boirie, Y.; Cruz-Jentoft, A.J.; Dicker, D.; et al. Definition and Diagnostic Criteria for Sarcopenic Obesity: ESPEN and EASO Consensus Statement. Obes. Facts 2022, 15, 321–335. [Google Scholar] [CrossRef]
- Woolcott, O.O.; Bergman, R.N. Defining cutoffs to diagnose obesity using the relative fat mass (RFM): Association with mortality in NHANES 1999–2014. Int. J. Obes. 2020, 44, 1301–1310. [Google Scholar] [CrossRef]
- García, C.G.; Almeida, J.M.G.; Aguilar, I.M.V.; Castañeda, V.B.; Guerrero, D.B. Morphofunctional assessment of patient nutritional status: A global approach. Nutr. Hosp. 2021, 38, 592–600. [Google Scholar] [CrossRef] [PubMed]
- Cuatrecasas, G.; De Cabo, F.; Coves, M.J.; Patrascioiu, I.; Aguilar, G.; March, S.; Balfegó, M.; Bretxa, C.; Calbo, M.; Cuatrecasas, G.; et al. Ultrasound measures of abdominal fat layers correlate with metabolic syndrome features in patients with obesity. Obes. Sci. Pract. 2020, 6, 660–667. [Google Scholar] [CrossRef] [PubMed]
- Torralvo, F.J.S.; Porras, N.; Fernandez, J.A.; Torres, F.G.; Tapia, M.J.; Lima, F.; Soriguer, F.; Gonzalo, M.; Martínez, G.R.; Olveira, G.; et al. Normative reference values for hand grip dynamometry in Spain. Association with lean mass. Hosp. Nutr. 2018, 35, 98–103. [Google Scholar] [CrossRef] [Green Version]
- Lin, M.-R.; Hwang, H.-F.; Hu, M.-H.; Wu, H.-D.I.; Wang, Y.-W.; Huang, F.-C. Psychometric Comparisons of the Timed Up and Go, One-Leg Stand, Functional Reach, and Tinetti Balance Measures in Community-Dwelling Older People. J. Am. Geriatr. Soc. 2004, 52, 1343–1348. [Google Scholar] [CrossRef] [PubMed]
- Dodds, R.M.; Syddall, H.E.; Cooper, R.; Benzeval, M.; Deary, I.J.; Dennison, E.M.; Der, G.; Gale, C.R.; Inskip, H.M.; Jagger, C.; et al. Grip Strength across the Life Course: Normative Data from Twelve British Studies. PLoS ONE 2014, 9, e113637. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cornejo-Pareja, I.M.; Gómez-Pérez, A.M.; Fernández-García, J.C.; Millan, R.B.S.; Luque, A.A.; Hollanda, A.; Jiménez, A.; Jimenez-Murcia, S.; Munguia, L.; Ortega, E.; et al. Coronavirus disease 2019 (COVID-19) and obesity. Impact of obesity and its main comorbidities in the evolution of the disease. Eur. Eat. Disord. Rev. 2020, 28, 799–815. [Google Scholar] [CrossRef] [PubMed]
- Moonen, H.P.F.X.; van Zanten, F.J.L.; Driessen, L.; de Smet, V.; Slingerland-Boot, R.; Mensink, M.; van Zanten, A.R.H. Association of bioelectric impedance analysis body composition and disease severity in COVID-19 hospital ward and ICU patients: The BIAC-19 study. Clin. Nutr. 2020, 40, 2328–2336. [Google Scholar] [CrossRef] [PubMed]
- Huang, Y.; Lu, Y.; Huang, Y.-M.; Wang, M.; Ling, W.; Sui, Y.; Zhao, H.-L. Obesity in patients with COVID-19: A systematic review and meta-analysis. Metabolism 2020, 113, 154378. [Google Scholar] [CrossRef] [PubMed]
- Cava, E.; Carbone, S. Coronavirus disease 2019 pandemic and alterations of body composition. Curr. Opin. Clin. Nutr. Metab. Care 2021, 24, 229–235. [Google Scholar] [CrossRef] [PubMed]
- Jensen, G.L.; Cederholm, T.; Correia, M.I.T.; Fukushima, R.; Higashiguchi, T.; Baptista, G.A.; Barazzoni, R.; Blaauw, R.; Coats, A.J.; Crivelli, A.; et al. GLIM Criteria for the Diagnosis of Malnutrition: A Consensus Report From the Global Clinical Nutrition Community. J. Parenter. Enter. Nutr. 2018, 43, 32–40. [Google Scholar] [CrossRef]
- Lee, Z.-Y.; Ong, S.P.; Ng, C.C.; Yap, C.S.L.; Engkasan, J.P.; Barakatun-Nisak, M.Y.; Heyland, D.K.; Hasan, M.S. Association between ultrasound quadriceps muscle status with premorbid functional status and 60-day mortality in mechanically ventilated critically ill patient: A single-center prospective observational study. Clin. Nutr. 2020, 40, 1338–1347. [Google Scholar] [CrossRef] [PubMed]
- Pardo, E.; El Behi, H.; Boizeau, P.; Verdonk, F.; Alberti, C.; Lescot, T. Reliability of ultrasound measurements of quadriceps muscle thickness in critically ill patients. BMC Anesthesiol. 2018, 18, 205. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Nakanishi, N.; Tsutsumi, R.; Okayama, Y.; Takashima, T.; Ueno, Y.; Itagaki, T.; Tsutsumi, Y.; Sakaue, H.; Oto, J. Monitoring of muscle mass in critically ill patients: Comparison of ultrasound and two bioelectrical impedance analysis devices. J. Intensiv. Care 2019, 7, 61. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Galli, A.; Colombo, M.; Carrara, G.; Luce, F.L.; Paesano, P.L.; Giordano, L.; Bondi, S.; Tulli, M.; Mirabile, A.; De Cobelli, F.; et al. Low skeletal muscle mass as predictor of postoperative complications and decreased overall survival in locally advanced head and neck squamous cell carcinoma: The role of ultrasound of rectus femoris muscle. Eur. Arch. Oto-Rhino-Laryngol. 2020, 277, 3489–3502. [Google Scholar] [CrossRef] [PubMed]
- Damanti, S.; Cilla, M.; Tuscano, B.; De Lorenzo, R.; Manganaro, G.; Merolla, A.; Pacioni, G.; Pomaranzi, C.; Tiraferri, V.; Martinenghi, S.; et al. Evaluation of Muscle Mass and Stiffness with Limb Ultrasound in COVID-19 Survivors. Front. Endocrinol. 2022, 13, 801133. [Google Scholar] [CrossRef] [PubMed]
- Umbrello, M.; Guglielmetti, L.; Formenti, P.; Antonucci, E.; Cereghini, S.; Filardo, C.; Montanari, G.; Muttini, S. Qualitative and Quantitative Muscle Ultrasound Changes in COVID-19 Related Ards Patients. Nutrition 2021, 91–92, 111449. [Google Scholar] [CrossRef] [PubMed]
- Goligher, E.C.; Dres, M.; Fan, E.; Rubenfeld, G.D.; Scales, D.C.; Herridge, M.S.; Vorona, S.; Sklar, M.C.; Rittayamai, N.; Lanys, A.; et al. Mechanical Ventilation–induced Diaphragm Atrophy Strongly Impacts Clinical Outcomes. Am. J. Respir. Crit. Care Med. 2018, 197, 204–213. [Google Scholar] [CrossRef] [PubMed]
- Reimers, K.; Reimers, C.D.; Wagner, S.; Paetzke, I.; Pongratz, D.E. Skeletal muscle sonography: A correlative study of echogenicity and morphology. J. Ultrasound Med. 1993, 12, 73–77. [Google Scholar] [CrossRef] [PubMed]
- Mayer, K.P.; Bastin, M.L.T.; Montgomery-Yates, A.A.; Pastva, A.M.; Dupont-Versteegden, E.E.; Parry, S.M.; Morris, P.E. Acute skeletal muscle wasting and dysfunction predict physical disability at hospital discharge in patients with critical illness. Crit. Care 2020, 24, 1–12. [Google Scholar] [CrossRef]
- Tang, X.; Huang, L.; Yue, J.; Qiu, L. Quantitative estimation of muscle mass in older adults at risk of sarcopenia using ultrasound: A cross-sectional study. Quant. Imaging Med. Surg. 2022, 12, 2498–2508. [Google Scholar] [CrossRef]
- Abe, T.; Thiebaud, R.S.; Loenneke, J.P.; Young, K.C. Prediction and validation of DXA-derived appendicular lean soft tissue mass by ultrasound in older adults. Age 2015, 37, 114. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Abe, T.; Loenneke, J.P.; Thiebaud, R.S. The use of ultrasound for the estimation of muscle mass: One site fits most? J. Cachex-Sarcopenia Muscle 2017, 9, 213–214. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Fukumoto, Y.; Ikezoe, T.; Taniguchi, M.; Yamada, Y.; Sawano, S.; Minani, S.; Asai, T.; Kimura, M.; Ichihashi, N. Cut-off Values for Lower Limb Muscle Thickness to Detect Low Muscle Mass for Sarcopenia in Older Adults. Clin. Interv. Aging 2021, 16, 1215–1222. [Google Scholar] [CrossRef] [PubMed]
- Battaglia, Y.; Ullo, I.; Massarenti, S.; Esposito, P.; Prencipe, M.; Ciancio, G.; Provenzano, M.; Fiorini, F.; Andreucci, M.; Storari, A.; et al. Ultrasonography of Quadriceps Femoris Muscle and Subcutaneous Fat Tissue and Body Composition by BIVA in Chronic Dialysis Patients. Nutrients 2020, 12, 1388. [Google Scholar] [CrossRef] [PubMed]
- Nijholt, W.; ter Beek, L.; Hobbelen, J.S.; van der Vaart, H.; Wempe, J.B.; van der Schans, C.P.; Jager-Wittenaar, H. The added value of ultrasound muscle measurements in patients with COPD: An exploratory study. Clin. Nutr. ESPEN 2019, 30, 152–158. [Google Scholar] [CrossRef] [PubMed]
- Abe, T.; Kawakami, Y.; Kondo, M.; Fukunaga, T. Comparison of ultrasound-measured age-related, site-specific muscle loss between healthy Japanese and German men. Clin. Physiol. Funct. Imaging 2011, 31, 320–325. [Google Scholar] [CrossRef] [PubMed]
- Deng, M.; Zhou, X.; Li, Y.; Yin, Y.; Liang, C.; Zhang, Q.; Lu, J.; Wang, M.; Wang, Y.; Sun, Y.; et al. Ultrasonic Elastography of the Rectus Femoris, a Potential Tool to Predict Sarcopenia in Patients With Chronic Obstructive Pulmonary Disease. Front. Physiol. 2022, 12, 783421. [Google Scholar] [CrossRef] [PubMed]







{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Participants (n = 30) | |
|---|---|
| Age (years) | 60 ± 9.4 |
| Male n (%) | 23 (76.7) |
| BMI (kg/m2) | 31.6 ± 7.4 |
| ICU stay (days) | 10 ± 16.5 |
| Hospital stay (days) | 23 ± 19.9 |
| Stress hyperglucemia (%) | 73.3 |
| Mechanical Ventilation (%) | 53.3 |
| Manoeuvres prone (%) | 46.7 |
| Corticosteroid Therapy (%) | 83.3 |
| Home oxygen therapy after hospital admission (%) | 53 |
| Comorbidities | |
| Diabetes Mellitus (%) | 26.7 |
| Arterial Hypertension | 53.3 |
| Dyslipidaemia (%) | 43.3 |
| Obesity by BMI ≥ 30 kg/m2(%) | 63.3 |
| Independent Variables | Standardized β | 95% CI | p |
|---|---|---|---|
| Length of ICU stay | 0.636 | 0.026, 0.148 | 0.007 * |
| Mechanical ventilation | −0.554 | −4.308, −0.594 | 0.012 * |
| Age | −0.323 | −0.149, −0.006 | 0.035 * |
| Sex | −0.260 | −3.048, 0.340 | 0.112 |
| Overall Median (Interquartile Range) | Male (n = 23) Median (Interquartile Range) | Female (n = 7) Median (Interquartile Range) | p ª | ||
|---|---|---|---|---|---|
| MUSCLE ASSESSMENT | |||||
| Quantitative parameters | |||||
| Cross-sectional area (cm2) | 4.35 (3.5–5.33) | 4.76 (3.56–5.43) | 3.65 (2.80–3.89) | 0.025 | |
| Cross-sectional area/height (cm2/m) Cross-sectional area/weigh (cm2/Kg) | 2.54 (2.07–3.04) 0.050 (0.039–0.060) | 2.65 (2.11–3.16) 0.051 (0.041–0.060) | 2.24 (1.67–2.32) 0.037 (0.026–0.060) | 0.069 0.065 | |
| Muscle circumference | 9.43 (8.53–10.15) | 9.54 (8.73–10.30) | 8.61 (7.55–9.83) | 0.096 | |
| Muscle circumference/height (cm2/m) | 5.40 (4.93–5.93) | 5.42 (5.02–5.90) | 5.25 (4.58–6.03) | 0.532 | |
| Muscle thickness (Y-axis) | 1.38 (1.15–1.61) | 1.40 (1.15–1.63) | 1.22 (0.87–1.60) | 0.564 | |
| X-axis | 3.95 (3.35–4.24) | 3.99 (3.66–4.24) | 3.28 (2.69–4.48) | 0.266 | |
| Qualitative parameters | |||||
| Mean Echo intensity | 73.28 (50.69–81.8) | 69.09 (47.60–78.09) | 79.11 (56.98–93.15) | 0.296 | |
| Minimum echo intensity | 12 (0.25–27) | 12 (0–24.5) | 12 (5–34) | 0.321 | |
| Maximum echo intensity | 184 (176.25–203.75) | 187 (177–207.5) | 177 (170–196) | 0.090 | |
| Leg | ADIPOSE TISSUE ASSESSMENT | ||||
| Subcutaneous Adipose tissue | 0.76 (0.50–1.49) | 0.71 (0.47–0.83) | 1.66 (1.21–1.80) | 0.007 | |
| Abdomen | Total subcutaneous adipose tissue | 1.80 (1.30–2.60) | 1.65 (1.02–2.35) | 2.98 (1.75–3.72) | 0.008 |
| Superficial subcutaneous adipose tissue | 0.84 (0.57–1.27) | 0.75 (0.42–0.92) | 1.52 (0.99–2.09) | 0.002 | |
| Visceral preperitoneal adipose tissue | 0.70 (0.42–0.87) | 0.70 (0.43–0.86) | 0.69 (0.38–0.90) | 0.917 |
| SKELETAL MUSCLE INDEX (SMI) ESTIMATED | ||||
|---|---|---|---|---|
| Algorithm 1 (Kg/m2) | R | R2 | SEE (Kg/m2) | p |
| Estimated SMI = 1.015 + 0.246 × RF-CSA (cm2) + 0.714 × BMI (Kg/m2)–0.433 × Sex (male:0/female:1) + 0.45 × Age (y). | 0.890 | 0.792 | 1.10 | <0.001 |
| Algorithm 2 (Kg/m2) | 0.880 | 0.774 | 1.14 | <0.001 |
| Estimated SMI = 1.006 + 0.193 × Y-axis (cm) + 0.711 × BMI (Kg/m2)–0.499 × Sex (male:0/female:1) + 0.08 × Age (y). | ||||
| Algorithm 3 (Kg/m2) | 0.925 | 0.856 | 0.92 | <0.001 |
| Estimated SMI = −1.584 + 0.369 × HGS (Kg) + 0.820 × BMI (Kg/m2)–0.403 × Sex (male:0/female:1) + 0.155 × Age (y). | ||||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Cornejo-Pareja, I.; Soler-Beunza, A.G.; Vegas-Aguilar, I.M.; Fernández-Jiménez, R.; Tinahones, F.J.; García-Almeida, J.M. Predictors of Sarcopenia in Outpatients with Post-Critical SARS-CoV2 Disease. Nutritional Ultrasound of Rectus Femoris Muscle, a Potential Tool. Nutrients 2022, 14, 4988. https://doi.org/10.3390/nu14234988
Cornejo-Pareja I, Soler-Beunza AG, Vegas-Aguilar IM, Fernández-Jiménez R, Tinahones FJ, García-Almeida JM. Predictors of Sarcopenia in Outpatients with Post-Critical SARS-CoV2 Disease. Nutritional Ultrasound of Rectus Femoris Muscle, a Potential Tool. Nutrients. 2022; 14(23):4988. https://doi.org/10.3390/nu14234988
Chicago/Turabian StyleCornejo-Pareja, Isabel, Ana Gloria Soler-Beunza, Isabel María Vegas-Aguilar, Rocío Fernández-Jiménez, Francisco J. Tinahones, and Jose Manuel García-Almeida. 2022. "Predictors of Sarcopenia in Outpatients with Post-Critical SARS-CoV2 Disease. Nutritional Ultrasound of Rectus Femoris Muscle, a Potential Tool" Nutrients 14, no. 23: 4988. https://doi.org/10.3390/nu14234988